
티스토리 뷰
Supine position
G/A with double lumen endotracheal tube(E-tube)
Supine position with right arm and left arm both adduction-tucked
skin prep & sterile draping (목부분 drape 잘해놓기, drape 떨어지면 안되니까 곡선 부분에서 접어서 잘 붙혀야 한다★)
무영등 맞추기 (직상방 하나, 우측 어깨 위에서 들어오게 하나★)
Abdominal procedure ))
- Xiphoid process 부터 umbilicus 직상방까지 midline incision
: recutus fascia와 linear alba, peritoneum 을 차례로 열어 복강 내에 진입
: muscle fiber 주행방향을 기준으로 midline 을 찾는다.
-. Xiphoid process 상방 2cm에서 umbilicus 상방 1cm 까지 midline laparotomy를 한 후 계속하여 linear alba와 peritoneum을 절개하여 abdominal cavity를 노출시켰다.
: Xiphoid process 상방으로 더 크게 열어, 이후 esophagus 박리할 때 너무 깊게 느껴지지 않도록 하였다.(★)
- Bookwalter retractor를 설치
: 왼쪽은 좀 더 위쪽으로 설치하여 stomach 이 보일 수 있게 설치한다.
- 먼저 liver dome 과 rectal shelf, 복강의 각 사분획을 palpation
: metastastic nodule이 없음을 확인
- Kelly blade 두 개를 양 쪽 subcostal cartilage에 걸어 양측으로 traction 하면서 복강을 좌우측으로 벌리고
(prn. left lobe와 duodenum 1st part와의 일부 adhesion band를 제거한 다음) deaver를 설치하여 liver 의 left lobe을 우측으로 traction
- Peritoneal cavity의 seeding, ascites, adhesion 여부를 확인(liver도 확인한다)
- Spleen을 왼손으로 끌어잡아 올린 다음 spleen 뒤쪽 (옆쪽이 아닌 뒤쪽★) space에 wet OR gauze 2ea packing
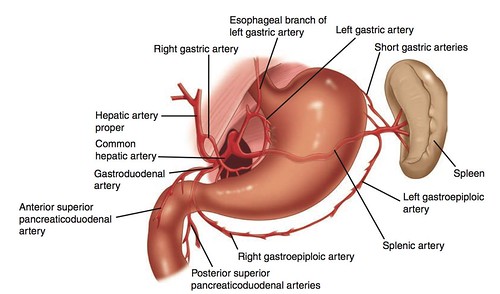
- Greater omentum division
: operator의 왼손으로 right gastroepiploic artery 및 left gastroepiploic artery (arcade) 의 pulse를 느끼면서
artery arcade가 다치치 않게 주의하면서 (PRG insertion site suture 시에도 이 artery 가 다치지 않도록 조심한다.)
: fat 부분은 bovie electrocautery로 육안으로 확인되는 vessel은 Harmonic scalpel로 division
: Stomach과 colon 사이의 greater curvature omentum을 bovie electrocautery와 Harmonic scalpel을 이용하여,
또는 bovie electrocautery를 이용하여 분리
: Right gastroepiploic artery (RGEA)를 확인하고 stomach에서 먼쪽으로 약 2cm 가량 바깥쪽으로
avascular plane을 찾아 greater omentum division 을 시작하였고, 먼저 duodeum 방향으로 pylrous 까지 진행.
: 이후 LGEA 방향으로 진행하면서 short gastric artery 를 찾았다.
- Short gastric artery division
: right angled clamp로 양쪽을 잡은 후 중간은 Metzenbaum scissor로 cutting 각각의 right angled clamp를 vicryl 2-0로 tie
(힘조절 잘해서 해야한다, 너무 세게하면 vessel 이 찢어진다.★)
왼손 포셉 오른손 잡고
Lt. epiploic artery를 splenic artery 분지 이후 지점에서 right-angled clamp를 양쪽으로 잡고 그 가운데를 자른 다음 3-0 vicryl 이용하여 ligation 자르고 short gastric 자르고 GEP lig. 빼고 wet gauze 빼고 dry gauze 1장 넣고 Lessor omentum esophagus 따라 올라가서
instrument Rt angle 3-0 tii
왼손으로 펴면서 잡아 내린다.(나중에 Tie 할 때 조금씩 왼손 오무린다)
common gastric 옆 G1 떼고
프롤린으로 자른다. 가만히 있는다. 타이할때 손을 느슨하게 해준다. 모아진다..
Lt gastric v. 두개를 동시에 잡고 Rt angle 잡고 잡고 2-0 double ligation
- Esophageal hiatus partial dissection
- Lesser curvature omentum을 stomach 에서 박리한 후 lesser sac 에서 left gastric artery 기시부를 볼 수 있도록 시야를 확보
- 위 과정에서 esophagus hiatus 에서 lesser curvature 쪽으로 올 때 G1 LN (common hepatic node) dissection 을 시행하였으며,
시행 후 cysterna chyli 위치이기 때문에 prolene 5-0 로 rapair 할 수 있게 continuous suture 를 시행해 주었다.
- Left gastric vein division
: 3-0 vicryl 로 proximal & distal tie ligation & division
- Left gastric artery division
: 2-0 vicryl distal ligation , proximal을 2-0 & 3-0 vicryl double ligation 한 뒤 division (★)
(artery 와 vein 을 함께 division 하기도 한다.)
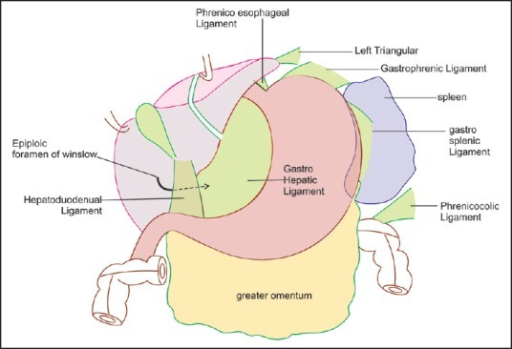
- Gastrohepatic ligament를 electrocautery를 이용하여 division 한 뒤 stomach의 posterior wall 과 retroperitoneum 사이를 박리하였고
left and right crus 및 periesophageal tissue를 dissection
(2nd assist가 narrow long deaver로 hiatus 주위 조직을 traction 하면서 진행하기도 하며,
Left gastric artery division 전에 시행하기도 한다.)
- Lesser curvature를 따라 Lt. gastric artery 4th branch 부터 proximal 방향으로 electrocautery & Harmonic scalpel 을 이용하여 박리.
: 먼저 bovie electrocautery를 이용해 lesser curvature의 viceral layer를 division 한 다음
right angled clamp로 isolation 하여 이 사이를 Harmonic scalpel로 Right angled clamp를 vicryl 2-0를 이용해 tie
(위 과정이 Right gastric artery division : proximal 을 2-0 vicryl tie ligation & division )
- Distal esophagus를 더 박리하였고 GE junction 주변을 박리하여 G3 (lesser curvature node), G4 (paracardial node) LN disseciton
(이 때 G3,G4 는 lesser curvature 에 붙어있다.)
: kelly clamp로 G3, G4 LN를 잡아 traction
: G3, G4 LN를 dissection 한 parahiatus esophagus 부위는 esophagus mucosa layer 의 vessel이 손상당하지 않도록
operator가 fine Debakey forcep으로 bleeding 이 있는 부분을 잡은 다음 1st assist가 Debakey forcep에 bovie electrocautery를
touch 하는 방법으로 bleeding control
- Pyloromyotomy
: Bovie power를 20으로 낮춘 뒤에 pylorus와 duodenum 과의 경계의 pylorus ring 을 확인 한 뒤에 duodenum 과의 경계에서
pylorus방향으로 3cm 가량의 vertical incision을 가하였다. Mixter clamp를 이용하여 stomach의 transverse muscle layer 아랫쪽으로
Mixter clamp를 집어 넣어 pyloric ring을 들어 올리면서 electrocautery를 이용하여 release 하였으며,
submucosa layer가 손상받지 않도록 주의하였다.
이 때 1st assist가 operator 잡은 Mixter 의 soft tissue 부분, 즉 1st assist 쪽의 부분을 cauterization 하였다.(★)
Muscle layer를 release 한 후에 pylorus ring을 구성하는 muscle의 양쪽을 partial incision 하는 pyloromyotomy를 시행
: Pyloromyotomy 부위에 Surgicel 35mm 1ea apply
mosquito 사이가 아니라 잡은 부위 위쪽에 bovie 가한다.
- Feeding jejunostomy
: jejunum treitz ligament 40cm distal portion 에 3-0 silk 2ea 로 double layer purse-
string suture 시행한 뒤 ( 이 때 1st assistant 는 CR 을 끊을 수 있게 도왔다.★) , Kocher 로
Lt. abdominal wall 을 잡고 mess 로 skin incision 을 만들어, bovie - mosquito - Kelly 로
벌리고 Foley 20Fr. insertion 하였다.
그 뒤 bovie 로 jejunum 을 opening 하고 (1st assist 는 jejunum 한쪽을 손으로 잡고,
suction 을 들고 assist★) foley 를 opening 에 넣고 끝까지 넣고 첫번째 purse-string siik 를
tie 한 뒤, 두번째 purse-string siik 는 operator 가 mosquito로 foley 를 당긴 뒤 tie 하였다.
(이 때 tie 가 너무 느슨해서도, 너무 tight 해서도 안되게 힘조절을 잘 해야 한다.★) 이 후 3-0
dermalone 으로 abdominal wall 에 360' circular tagging suture 시행한다.
(이 때 1st assistant 는 dermarone 을 각각 mosquito로 잡아주었다.★)
이 과정에서 foley 가 잘 들어가지 않을 경우 enema syringe 를 통하여 bowel lumen 을 넓혀주었다.
그렇지 않을 경우 2cc syringe 뚜껑을 이용하여 foley catheter 를 막아주었다.
- Meticulous bleeding control 후 bleeding 없음을 확인하고 Bookwalter self retractor를
제거하였다.
- Peritoneum은 vicryl 2-0를 이용해 continuous suture로 closure 하고
중간에 linear alba fascia suture를 vicryl 0 CR로 3회 interrupted suture(★)
- PDS #1 으로 linear alba fascia의 continuous suture를 시행한 다음 (죽을힘을 다해 위로 당겨야 한다.★)
subcutaneous, skin은 skin stapler를 이용해 closure 하였다.
Cervical procedure ))
- low collar incision
: platysma muscle layer 와 함께 cutting 해주었다. 1st assistant 는 에디슨 forcep 으로 operator 와
반대방향으로 같은힘을 주어 traction 해주었다.
(Kocher 로 위쪽 layer 를 수직으로 들면서(★) 박리를 하였다.)
이 후 시야확보를 위해 위쪽 layer 를 턱 위의 drape 에 tagging suture 해주었다. (풀리면 안된다★)
- Lt. side procedure
: SCM muscle medial border 를 따라 박리하여 omohyoid muscle 을 division 하여 LN IV, VI 를
노출하여 Neck LN #101 (Recurrent laryngeal node) dissection 하였으며 transverse cervical
artery 와 jugular vein 를 경계로 하여 subcuetaneous tissue 사이의 공간을 박리하여 Neck LN #103 (SCN node) dissection 을 시행.
- Rt. side procedure
: Lt. side 와 동일하게 LN dissection 을 진행하였다.
(위 과정은 operator 가 환자 오른쪽에 서서, Lt. SCN & Rt. RLN disseciton 을 시행하고
환자 왼쪽으로 이동하여 Rt. SCN & Lt. RLN dissection 을 시행하였다. )
- SCM muscle 을 simple suture 3번으로 layer를 맞춰준 뒤, platysma muscle 과 fascia layer를 함께(★)
interrupt suture 로 (knot 가 안쪽에 위치하도록★) closure 하였다.
- Subcutaneous, skin은 skin stapler를 이용해 closure 하였다.

Rt thoracotomy Thoracic procedure ))
- position change to left lateral decubitus position
(Pf. Choi)
- Eso-stomach 연결하기 위해 stomach에 EEA stapler 들어갈 opening 만들때, opening의 4분면에 각각 suture해서 EEA 넣고 실 잡아당김.
gastric conduit.. staple 치고 seromuscular reinforce할때 continuous로 함. proximal에서 시작하고 중간까지,
distal에서 다시 시작해서 중간까지하고 중간에서 tie. Gastric conduit을 mediastinum에 fixation 시키는 것을 매우 중요하게 여김.
- 4th intercostal space
- skin preparation & draping
- postero-lateral thoracotomy incision
: 환자의 scapular inferior angle 확인한 다음 surgical marker 를 이용해 scapular 하방의 1finger (2 to 3cm) 위치를 표시하였다.
Rib count를 하여 anterior axillary line, 5th ICS를 표시 한 다음 scapular posterior border와 thoracic spine의 paraspinal process의
midway를 표시하였다. 이 세 지점을 잇는 선을 그렸으며, 완만한 S자 모양의(조재일 교수님은 거의 C) 선을 완성하였다.
또한 이 선을 따라서 posterolateral thoracotomy incision
(등쪽에서는 spine 보다 scapula 에 붙혀서 insion 을 시행한다고 생각해야 한다★) serratus 절대 자르지 않고 undermining 안한다.

trapezium 자르지 않는다. 밑쪽으로 undermining 해야 벌어진다.
: latissimus dorsi를 division 하고 serratus anterior muscle의 aponeurosis를 cutting 하여 scapula 아래로 손을 집어넣어
spine 가까이에서 5th ICS의 위치를 확인하고 serratus anterior muscle 을 saving 하고 rhomboid muscle은 약 2cm 가량 cutting.
5th ICS 를 통하여 흉강 내로 진입하였으며, rib cutting은 시행하지 않았다. (시행하기도 한다.)
: 이 후 OR gauze 두 장으로 incision line 위 아래를 감싼 다음 rib sprader retractor 를 걸어 충분히 5th ICS을 벌렸다.
- Esophagus exposure & LN dissection
: Azygos arch 하방의 mediastinal plerua를 incision 하여 azygos arch 아래 쪽을 먼저 박리한 다음
lower esophagus를 박리하면서 8m LN를 dissection
: Lower esophagus를 온전히 박리하여 right angled clamp로 isolation 한 다음
penrose drain으로 걸어두고 Hiatus level 까지 충분히 박리하면서 LN #7 #8d dissection 을 시행하였다.
: Azygos arch 상방의 upper mediastinal pleura 를 esophagus 주행 위에서 vertical incision 하여 subclavian artery 아래 까지 division
: 계속하여 trachea 의 posterior side와 esophagus의 right side의 soft tissue를 dissection 하면서 상방으로 진행하여
right recurrent larygneal nerve(RRLN)를 확인하고 Metzenbaum scissor를 이용하여 sharp dissection 하여 RRLN LN dissection
Bachob clamp 로 upper thoracic esophagus를 잡아 retraction 하면서 esophagus를 dissection and release 하여 isolation 한 다음
걸어두었던 penrose drain을 posterior side와 anterior side로 당겨
esophagus를 anterior, posterior side로 traction 하면서 upper thoracic esophagus를 dissection
: Carina 근처의 mid thoracic esophagus 는 operator의 왼손으로 잡아 들어올리면서
주위 carina 및 left main bronchus 와의 plane 을 palpation 하면서 meticulous dissection 하여 분리.
: 다시 upper esophagus로 접근하여 mediastinal pleura를 blunt right angled clamp 로 잡아 retraction 하였다.
Esophagus를 들어 올리면서 trachea를 확인 후 1st assist가 suctiontip, tracheal retractor (두손으로 잡는다.★)를 이용해
trachea를 제쳤다. Left recurrent laryngeal nerve (LRLN) LN dissection 을 electrocautery를 이용하지 않고 Metzenbaum scissor를
이용하여 sharp dissection 하였다.
- Thoracic inlet level에서 prolene 2-0를 이용하여 purse string suture 를 한 뒤 mosquito 로 잡아
두고 (★) 약 1.5cm 하방에 bovie electrocautery로 vertical incision을 넣고 (한손에 forcep 한손에 suction 을 들고
gastric juice 를 빨면서 counter traction 을 잘 해준다 ★) mucosa까지 esophagus의 whole layer를 잡아 양쪽으로 벌리면서
마취과에 지시해 L-tube withdrawal 이 후 silk 로 vertical incision 에 full layer 를 simple suture 해주고 mosquito 로 잡아둔다. (★)
- Betadine ball 로 lumen 안을 닦아낸 다음 simple suture 하였던 실을 당기면서 Autosuture DST EEA 28mm: Anvil을 삽입한 후
이 실을 제거하였다. (needle 있는 쪽 실을 잡아당긴다) purse string 을 tie 하여 조여 둔 후 실 mosquito로 잡아 두고 purse string
직 하방에서 curved metzenbaum scissor 를 사용하여 esophagus transection 하였다.
- 이 후 distal resection margin을 1st assist가 Debakey forcep으로 mucosa를 포함해
serosa 양쪽 끝을 평평하게 될 수 있도록 잘린부분과 그 반대쪽 끝을 잘 잡은 뒤
(위 과정에서 curved metzen 으로 잘리는 것을 확인한 뒤 바로 forcep 두개를 들고 기다리자. incision 넣어서 잘린 부분을 모아서 잡고,
반대쪽을 잡는다 ★) Mayo scissor로 잘라 frozen biopsy를 시행
- 미리 mobilization 하였던 stomach을 pleural cavity 내로 pull up 하였다. Anvil을 다시 betadine ball로 소독 한 뒤 guaze packing 하여
두고 esophagus의 transection margin 은 long kelly로 잡은 후 betadine ball 로 소독한 후 다시 gauze로 lumen 을 감싼 후 kelly
로 다시 잡아 두었다.
- Bovie electrocautery를 이용하여 cardiac opening을 만들어
(한손에 forcep 한손에 suction 을 들고 gastric juice 를 빨면서 counter traction 을 잘 해준다★)
Autosuture DST EEA 28mm instrument를 밀어 넣고 knob를 반시계 방향(★)으로 돌려 trochar가
stomach fundus을 뚫어 esophagogastrostomy 될 opening을 만들어 주었다.
- Anvil과 instrument를 결합시킨 후 녹색 indicator가 나타날 때까지 knob를 시계 방향(★)으로 돌려서 approximation 한 후
fire 하여 anastomosis 를 완성하였다. 이 때 1st assist 가 mediastinal pleura를 traction 하여 anastomosis site에 pleura가
끼지 않게 하였다. Knob을 반시계 방향으로 돌려서 Anvil을 푼 후 기구를 cardiac opening을 통해 제거하였다.
- Anvil 내의 proximal resection margin을 blade #15를 이용해 제거 ( blade를 썰지 않고 민다.★) 한후 permanent biopsy 검체로 보냈다.
Opening을 통해 anastomosis site에 color 괜찮은지 확인한 뒤bleeding이 없는 것을 확인 후 L-tube 를 50cm 까지 밀어 넣고 고정하였다.
- Cardiac opening 부위를 New TA DST Series 90-4.8mm 1ea를 이용하여 stapling 하고 나서 분리하여 cardia와 esophagus를 적출
마취과에 지시해 L-tube 를 55cm까지 밀어넣고, L-tube tip이 stomach 안에 있음을 operator의 손가락으로 직접 촉지하여 확인.
- Stapling site는 PRN) vicryl 3-0 CR로 interrupted seromuscular suture를 하여 reinforcement.
Vicryl 3-0 CR로 mediastinal pleura를 esophagogastrostomy 부분에서 suture 하여 cover.
- Warm saline으로 irrigation 후 마취과에 지시해 two lung ventilation을 시행하였다.
Expansion 잘 됨을 확인하고 meticulous bleeding control 후 bleeding 없음을 확인
- 28Fr straight chest tube 1ea를 anterior axillary line, 8th ICS로 insertion 하였고, apex 직하방에 위치시켰다.
(고정하는 실과 purse-string suture 하는 실을 길이를 잘 가늠해서 자르고 mosquito 로 물어둔다★)
흉강 내에 거치하는 tube 끝에 side hole을 뚫어 air vent 및 drainage를 좋게 하였다.
(이때 mosquito 로 잘리는 chest tube 부분을 잡아준다★)
- Vicryl #0 4개를 이용해 figure of eight 으로 rib reapproximation을 시행하였고
(이때 intercostal muscle 들이 제자리에 딱 맞게 들어갈 수 있도록 forcep으로 위치를 잡아주어여 한다★)
마취과에 지시해 two lung ventilation을 하게 하여 lung이 잘 expansion 되는 것을 확인
하였다. Pericostral suture를 시행하고, muscle, fascia를 layer by layer로 closure
/ Subcutaneous, skin 은 skin stapler로 closure
- 수술을 종료하고 double lumen E-tube 를 single lumen E-tube 로 change 하고 환자의
vital sign을 monitoring 하면서 환자를 TS ICU로 이송하였다.
수술기록 정리
Peritoneal cavity : No adhesion
No ascites
No seeding
Palpable nodules in rectal shelf (No)
Hepatomegaly (No) Splenomegaly (No)
Pleura : Rt. No adhesion
No effusion
No seeding
Condition of esophageal substitute
Stomach - Length : Sufficient
- Blood flow after preparation : Good
Number of lesions : 1
ㆍLesion 1 - Size : 5×5cm
(main)
- Location : Thoracic - Lower
- Invasion of surrounding tissue : None
LN stations : LN enlargement - None
Extranodal invasion - None
LN dissection - Abdominal G1 G2 G3
Mediastinal RRLN LRLN 7 8U
Resection margin : R0
<abd.>
1. laparoscopic 5 port
- zyphoid, above umbilicus 5mm
(umbilicus skin 을 들어올리고 5mm port 후 CO2 gas insert)
- Lt. cartilage(upper) 12mm
- Lt. lower, Rt. lower 5mm
2. perotoneal cavity에서 ascites, seeding, rectal shelf 확인
3. harmonic scalpel 사용하여 greater omentum과 lesser omentum을 박리
4. LN #G1, G2, G3 dissection, G3 division with endoGIA 60*purple
5. Lt. gastric a. cutting with endoGIA 45*tan
6. pyloromyotomy : endostitch
<thorax>
7. VATS port & CO2 gas on
- 3th ICS 5mm
- 6th ICS 5mm*2
- 8th ICS 5mm
8. pleural cavity에서 pleural adhesion, effusion, seeding 확인
9. azygos v. division with endoGIA 45*tan
10. LN #RRLN, 8 dissection
11. LN #7, LRLN dissection
<abd.>
1. laparoscopic 5 port
- zyphoid, above umbilicus 5mm
(umbilicus skin 을 들어올리고 5mm port 후 CO2 gas insert)
- Lt. cartilage(upper) 12mm
- Lt. lower, Rt. lower 5mm
2. perotoneal cavity에서 ascites, seeding, rectal shelf 확인
3. harmonic scalpel 사용하여 greater omentum과 lesser omentum을 박리
4. LN #G1, G2, G3 dissection, G3 division with endoGIA 60*purple
5. Lt. gastric a. cutting with endoGIA 45*tan
6. pyloromyotomy : endostitch
<thorax>
7. VATS port & CO2 gas on
- 3th ICS 5mm
- 6th ICS 5mm*2
- 8th ICS 5mm
8. pleural cavity에서 pleural adhesion, effusion, seeding 확인
9. azygos v. division with endoGIA 45*tan
10. LN #RRLN, 8 dissection
11. LN #7, LRLN dissection
12. EEA 25mm,
gastric tubing with endoGIA 60*purple*2, 45*purple
13. stomach을 pleural cavity 내로 pull up,
G3 division with endoGIA 60*purple,
14. mediastinal pleura closure with endostitch
15. CTD 28Fr.
<<수술과정>> Thoracic surgery atlas와 비교해서 공부해보자
Position : Supine position
-> Lateral decubitus position( Lt. )
Esophagectomy : Transthoracic Rt. (Near total thoracic esophagectomy)
Abdominal procedure
Approach : Laparoscopy
Kocher maneuver ( Yes)
Great omentum resection : Partial with RGEA preparation
with Harmonic scalpel
Lesser omentum resection
Crus muscle division ( Yes)
Lt. gastric artery division ( Yes)
Esophageal substitute
- Whole stomach
Route :Posterior mediastinal
Gastric drainage procedure : Pyloromyotomy
Feeding jejunostomy : No
Thoracic procedure
Approach : VATS
Bronchial artery saving ( No)
Azygos vein division ( Yes)
Thoracic esophagectomy : Full above carina
Intrathoracic anastomosis
- End-to-end with Stapler ( EEA 25 )
Above the carina
Completion of anastomosis
- Flexible Endo-stapler
Recurrent laryngeal nerve saving ( Rt.Lt. )
Drain insertion : Chest tube ( Rt.)
Lymphadenectomy : 2-field LN dissection (Abdominal + Thoracic)
Pain control method : Epidural PCA
Joint op. : No
1. anethesia : GA
2. supine position 후
3. laparoscopic 5 port 시행하였다.
- zyphoid, above umbilicus 5mm (umbilicus skin 을 들어올리고 5mm port 후 CO2 gas insert)
- Lt. cartilage(upper) 12mm
- Lt. lower, Rt. lower 5mm
4. perotoneal cavity 내에 adhesion이나 seeding, rectal shelf 에 이상없음
확인하였다.
5. spleen, stomach 에 특별한 lesion은 없었다.
6. harmonic scalpel 사용하여 greater omentum 부터 박리하여
RGEA 주행 확인하면서 RGEA를 확보하였다. LGEA 및 short gastric a. 정리하였다.
stomach을 위로 들어올려 pancreas와 dissection 하였다.
7. lesser omentum 박리 후 Rt. crus m.을 forcep 으로 제끼면서 주변 tissue 를 박리하고
lesser curvature 중간에서 Rt. gastric a. branch 정리 후 LN #G1, G2, G3 dissection 하였
다.
8. Lt. gastric a. prox.은 endoGIA 45*tan으로 cutting 시행하였다.
9. 추가로 LN# G3 division with endoGIA 60*purple 하고
pyloromyotomy(endostitch로 양쪽을 tie 후 들어올리고 bovie pressure 20으로 진행) 및
histus, Lt. crus m. 추가 박리 후
10. abd. wound closure 하였다.
11. position change to lt. lat. decubitus position 하고
12. VATS port & CO2 gas on 시행하였다.
- 3th ICS 5mm
- 6th ICS 5mm*2
- 8th ICS 5mm
13. pleural cavity에서 특별한 adhesion이나 lesion은 없었다.
14. azygos v.을 endoGIA 45*tan으로 division 하고 bronchial a.는 cauterization 한 후
upper esophagus에 u-tape 을 걸고 bovie로 박리하였다.
15. tracheal 를 제끼면서 LN #RRLN, 10L박리하였다.
16. esophagus 아래쪽으로 이동하면서 박리를 계속하여 LN #7, LLRN 박리하였다.
17. 6th ICS port를 이어서 utility port를 만들고
Thoracic inlet level 조금 아래에서 prolene #2-0를 이용하여 purse string
suture 를 한 뒤 약1.5cm 하방에 bovie electrocautery로 vertical incision을 넣고
mucosa까지 esophgus의 whole layer를 잡아 양쪽으로 벌리면서 L-tube withdrawal 하였다.
18. EEA 25mm 의 Anvil을 삽입하고 purse string
을 tie하여 조여 둔 후 purse string 직하방에서
esophagus를 transection 하였다.
19. stomach을 pleural cavity 내로 pull up 하여 G3를 endoGIA 60*purple로 division 하여
박리하였다.
20. anastomosis 시행할 stomach fundus에 marker로 표시하고 4방향 suture 및 bovie를
이용하여 cardiac opening을 만들어 utility port 안으로 다시 넣고
EEA 25mm instrument를 밀어 넣고 trochar 를 반시계 방향으로 돌려 trochar가 stomach
fundus을 뚫어 esophagogastrostomy 될 opening 을 만들어 주었다.
21.Anvil과 instrument를 결합시킨 후 시계 방향으로 돌려서 approximation 한 후 fire하여
anastomosis를 완성하였다.
22. Anvil내의 proximal resection margin permanent bx. 의뢰하고
endoGIA 60*purple*2, 45*purple를 이용하여 stapling하고 나서 분리하여
cardia와 esophagus를 적출해 내었다.
23. frozen bx. of proximal margin 결과 negative for malignancy 소견 보고받고
esophagus를 mediastinal pleura로 덮으면서(with endostitch) 고정하였다.
24. warm saline irrigation 및 two lung ventilation을 시행하면서 이상없음 확인하고
25. 28Fr. CTD를 8th ICS에 넣고 azygos v. level에 위치 하여 고정 후 wound
closure 하였다.
1. anethesia : GA
2. supine position 후
3. laparoscopic 5 port 시행하였다.
- zyphoid, above umbilicus 5mm
(umbilicus skin 을 들어올리고 5mm port 후 CO2 gas insert)
- Lt. cartilage(upper) 12mm
- Lt. lower, Rt. lower 5mm
4. perotoneal cavity 내에 adhesion이나 seeding, rectal shelf 에 이상없음 확인하였다.
5. Spleen, stomach 에 특별한 lesion은 없었다.
6. harmonic scalpel 사용하여 greater omentum 부터 박리하여 RGEA 주행 확인하면서 RGEA를 확보하였다. LGEA 및 short gastric a.
정리, stomach을 위로 들어올려 pancreas와 dissection 하였다.
7. Lesser omentum 박리 후 Rt. crus m.을 forcep 으로 제끼면서 주변 tissue 를 박리하고 lesser curvature 중간에서
Rt. gastric a. branch 정리 후 LN #G1, G2, G3 dissection 하였다.
8. Lt. gastric a. prox.은 endoGIA 45*tan으로 cutting 시행하였다.
9. 추가로 LN# G3 division with endoGIA 60*purple 하고
pyloromyotomy(endostitch로 양쪽을 tie 후 들어올리고 bovie pressure 20으로 진행) 및 hiatus, Lt. crus m. 추가 박리 후
10. Abd. wound closure 하였다.
11. position change to lt. lat. decubitus position 하고
12. VATS port & CO2 gas on 시행하였다.
- 3th ICS 5mm
- 6th ICS 5mm*2
- 8th ICS 5mm
13. pleural cavity에서 특별한 adhesion이나 lesion은 없었다.
14. azygos v.을 endoGIA 45*tan으로 division 하고 bronchial a.는 cauterization 한 후 upper esophagus에 u-tape 을 걸고 bovie로 박리.
15. tracheal 를 제끼면서 LN #RRLN, 10L박리하였다.
16. esophagus 아래쪽으로 이동하면서 박리를 계속하여 LN #7, LLRN 박리하였다.
17. 6th ICS port를 이어서 utility port를 만들고 Thoracic inlet level 조금 아래에서 prolene #2-0를 이용하여
purse string suture 를 한 뒤 약 1.5cm 하방에 bovie electrocautery로 vertical incision을 넣고 mucosa까지
esophgus의 whole layer를 잡아 양쪽으로 벌리면서 L-tube withdrawal 하였다.
18. EEA 25mm 의 Anvil을 삽입하고 purse string
을 tie하여 조여 둔 후 purse string 직하방에서
esophagus를 transection 하였다.
19. stomach을 pleural cavity 내로 pull up 하여 G3를 endoGIA 60*purple로 division 하여
박리하였다.
20. anastomosis 시행할 stomach fundus에 marker로 표시하고 4방향 suture 및 bovie를
이용하여 cardiac opening을 만들어 utility port 안으로 다시 넣고
EEA 25mm instrument를 밀어 넣고 trochar 를 반시계 방향으로 돌려 trochar가 stomach
fundus을 뚫어 esophagogastrostomy 될 opening 을 만들어 주었다.
21.Anvil과 instrument를 결합시킨 후 시계 방향으로 돌려서 approximation 한 후 fire하여
anastomosis를 완성하였다.
22. Anvil내의 proximal resection margin permanent bx. 의뢰하고
endoGIA 60*purple*2, 45*purple를 이용하여 stapling하고 나서 분리하여
cardia와 esophagus를 적출해 내었다.
23. frozen bx. of proximal margin 결과 negative for malignancy 소견 보고받고
esophagus를 mediastinal pleura로 덮으면서(with endostitch) 고정하였다.
24. warm saline irrigation 및 two lung ventilation을 시행하면서 이상없음 확인하고
25. 28Fr. CTD를 8th ICS에 넣고 azygos v. level에 위치 하여 고정 후 wound
closure 하였다.
Frozen biopsy : Resection margin (negative for malignancy)
조직검사 : Yes
Drainage : 28Fr. in rt. thorax
Supine position에서 마취를 시작하고 double lumen e-tube를 삽입한 후 a-line을 삽입했다. L-tube를 삽입하여 55cm에서 L-tube 고정했다.
1. Abdominal phase
shoulder roll를 삽입하여 neck extension position을 취하고 chlorohexidine soaping 후 chlorohexidine-alcohol solution으로 피부소독을 한 후 sterile draping을 했다. Xiphoid process 상방 2cm에서 umbilicus 상방 1cm 까지 midline laparotomy를 한 후 계속하여 linear alba와 peritoneum을 절개하여 abdominal cavity를 노출시켰다. rectal shelf와 liver dome, 복강 각 사분획과 splenic dome을 palpitation 하였고 seeding, ascite, adhesion은 없었다. Bookwalter retractor (kelly x 2, Deaver x 1)를 거치했다. 위의 cardia와 lessor curvature 에 촉지되는 종괴는 없었다. spleen bed에 wet OR gauze 2장을 넣어 spleen을 elevation 하였다. Stomach greater curvature를 따라 stomach과 2cm 가량 간격을 두고 greater omentum 의 midline 정도에서 avascular plane을 따라 bovie electrocautery로 절개를 하고 epiploic vessel은 thunderbeat 를 이용하여 절단하면서 duodenum 방향으로 진행하였다. 위의 posterior wall과 retroperitoneum과의 gastrosplenic ligament를 절개하면서 RGEA의 origin과 pulse를 확인하였고 다시 fundus 방향으로 진행하여 omentum을 계속 division 하였고 LGEA를 splenic artery 에서 분지 이후 지점에서 right-angled clamp를 양쪽으로 잡고 그 가운데를 자른 다음 각각의 끝을 3-0 vicryl 를 이용하여 ligation 하였다. Fundus까지 박리를 진행하고 계속하여 short gastric artery를 thunderbeat를 이용하여 division 하였다. Spleen bed의 OR gauze는 dry OR gauze 한장으로 바꿨다. 이어서 계속 반시계 방향으로 esophageal hiatus와 abdominal esophagus 의 경계 부위를 bovie 로 incision을 가한 후 왼쪽 편에서 내부의 esophagus 주위 ligament를 충분히 release 하였다. Gastrohepatic ligament의 avascular plane에 incision을 가하고 incision을 right crus까지 연장하여 hiatus 우측을 노출하였다. Long-narrow Deaver를 hiatus 상방에 위치시켜 traction 하였고 hiatus를 통해 4FB가 들어갈 정도로 공간을 확보하고 식도를 mobilization 시켰다. 조심스럽게 esophagus 에 부착된 상태로 주위를 dissection 하여 분리 하였다. Long-narrow Deaver로 hiatus를 anterior로 traction 하고 동시에 Deaver로 hiatus를 left side로 traction 하여 공간을 충분히 확보하였다. Hiatus를 통해 식도를 충분히 mobilization 시켰다. Stomach을 등쪽으로 누르면서 아래쪽으로 살짝 당겨 젖히면서 lesser sac 내의 common hepatic artery 주위를 박리하여 G1를 채취했다. G1 node의 enlargement는 없었다. Prolene 4-0 로 박리 부위를 주위 tissue를 모아 봉합하여 cover 하였다.
이어 Left gastric vessel을 박리하여 먼저 left gastric vein 근위부 주위를 clearing 한 이후 근위부와 원위부에 각각 right-angled clamp를 잡아 절단하고 Vicryl 2-0를 이용하여 각각 ligation 하였다. 같은 방법으로 Left gastric artery 주위를 clearing 한 뒤 right-angled clamp 두 개를 각각 vessel 근위부와 원위부에 잡고 절단한 다음 원위부를 2-0 Vicryl로 ligation 하고 근위부를 2-0 와 3-0 Vicrl 로 double ligation 하였다. 남은 gastrohepatic ligament를 electrocautery를 이용하여 절제하고 stomach의 posterior wall 과 retroperitoneum 사이를 박리하고 위를 모두 mobilization 하였다. Lesser curvature에서 Rt. Gastric artery 의 위치를 확인하고 3rd branch 원위부에서 lesser omentum을 위 방향으로 bovie electrocautery로 절개한 다음 노출된 right gastric artery 근위부는 right angled clamp로 잡고 3-0 vicryl ligation 하고 원위부는 Kelly clamp로 잡았다. 마취과에 지시해 Levin tubue를 35cm 까지 withdrawal 하였다. TCT75 2개를 이용하여 right gastric artery 3rd branch 이후의 lesser curvature에서 fundus 방향으로 위를 곧게 늘어뜨리면서 cardia의 mass를 절단면에 충분히 margin을 두고 포함하게 하면서 stapling & Division 하여 gastric tube를 만들었다. Fundus 주변은 남겨두어 thoracic phase 에서 마무리하도록 하였다.
Gastric tube를 목까지 늘어뜨려 길이를 확인하고 division 된 distal esophagus에서 lesser omentum을 잘라내어 G3, G4 LN로 분리하여 병리 검체로 보냈다. Bovie를 20W로 낮춘 뒤 pylorus ring을 확인하고 stomach에서 duodenum의 경계까지 pylorus ring 위를 2cm 가량 vertical incision을 가하였다. Stomach의 transverse muscle layer 아래쪽으로 Mixter clamp를 집어넣어 pyloric ring을 들어올리면서 electrocautery를 이용하여 절개하여 release 하였으며, submucosa layer cutting edge를 bleeding control 한 다음 Surgicel 을 부착하여 pyloromyotomy를 완성하였다. Gastric tube의 stapling line을 원위부에서 근위부 방향으로 seromuscular layer를 vicryl 3-0 CR을 이용하여 interrupted Lembert suture 하여 보강하였다.
2. Feeding jejunostomy
Treitz ligmament 하방 30cm 부위 3rd loop의 jejunum에 Vicryl 3-0 CR를 이용하여 2개의 inner & outer purse string suture 하고 Mosquito clamp 로 실을 물어 두었다. Left paraumblical area 에 5mm 정도의 incision을 넣고 Richardson reractor로 좌측 복벽을 들어올린 후 20Fr foley catheter 를 삽입하고 복벽 밖으로 2nd assistant가 foley catheter를 잡아 복벽 밖으로 꺼내들었고 Jejunum의 purse string 주위를 들어올려 purse string 가운데에 bovie로 incision을 가한 뒤 mosquito로 벌리고 안쪽 lumen 을 확인하면서 hole을 suction 하였다. Foley catheter를 dl 구멍 사이로 삽입 후 끝에 연결되어 있던 enema syringe 로 20cc 정도의 공기를 넣어 jejunum 안쪽 lumen이 잘 부풀어 오르는지, foley catheter의 끝 위치를 확인하였다. 다시 공기를 뺀 후 purse string suture를 inner suture부터 tie 하고 tie 하면서 jejunum의 mucosa가 노출되지 않도록 seromuscular layer를 foley catheter에 붙여 inversion 시켰다. Jejunum과 abdominal wall에 Vicryl CR 4개를 이용하여 360도로 suture 한 뒤 tie하여 고정하였다. Foley catheter는 Nylon 3-0로 stay suture를 시행해 고정했다. Bleeding이 없음을 확인 후 L-tube가 gastric tube에 잘 들어와 있는 것을 확인하였다. Peritoneum은 vicryl 2-0를 이용해 continuous suture로 closure 하고 PDS로 linea alba fascia를 continuous suture closure 하고 skin stapler로 skin closure 하였다.
3. Thoracic phase
Left lateral decubitous position을 취한 후 피부 소독을 하고 sterile draping 하였다. 환자의 surface anatomy를 확인했다. Inferior angle of scapula를 확인하고 여기에서 2FB 아래 부위 표시 했다. 12th rib 부터 늑골을 count 하여 5th intercostal space 에 위치를 확인하였다. Lateral incision line 은 직선으로 anterior end는 5th ICS를 향하게 하였고 inferior angle of scapula에서 posterior 쪽은 spine과 scapula의 medial border 가운데에서 incision line을 그렸고 incision line을 따라 posterolateal thoracotomy incision을 하였다. Latissimus dorsi 를 절개하고 serratus anterior의 aponeurosis를 절개했다. Scapula 아래로 왼손을 집어 넣어 spine에 가까이에서 5th ICS 위치를 확인하고 trapeziums muscle을 2cm 가량 절개했다. 5th ICS를 6th rib에 바짝 붙여 parietal pleura를 절개하였다. Dry OR gauze를 반으로 접어 5th ICS 위 아래 늑골에 댄 다음 조금씩 spreader를 벌렸고, 그 사이 흉강내 유착을 제거하였다. Lung 사이의 유착을 제거하였다. 이어서 azygos arch 아래에서 esophagus 위의 mediastinal pleura를 식도 장축 방향으로 절개한 다음 흉부 식도 mobilization을 시작하였다. Penrose drain을 식도에 걸어 Kelly clamp로 문 다음 anterior 또는 posterior로 당기ㅂ면서 Lower thoracic esophagus를 mobilization 하였다. 이 과정에서 azygos arch 근처에서 LN8 (middle)을 박리했다. 박리중 노출되는 esophageal artery도 thunderbeat를 이용하여 resection 하였고 lower esophagus에서 LN8 (lower)를 박리했다. Esophageal hiatus까지 충분히 lower thoracic esophagus를 mobilization 한 다음 azygos arch 아래의 mid-thoracic esophagus를 mobilization 하였다. Upper mediastinal pleura를 esophagus 주행 위에서 vertical incision을 하여 subclavian artery 아래까지 incision을 한 다음 계속해서 trachea의 posterior side와 esophagus의 Rt. Side의 soft tissue를 dissection 하면서 상방으로 진행하여 LN8 (upper) 를 절제 하였다. 박리 중 trachea 측면의 vagus nerve 주행과 subclavian artery에서 이 branch의 right recurrent laryngeal nerve를 확인하고 주위 LN는 모두 절제한 것을 확인하였다. Azygos arch 상방에서 arch 하방을 박리하여 아래쪽 식도에 있던 penrose drain을 right-angled clamp로 잡아 양 끝을 azygos arch 상방으로 올린 다음 다시 Kelly clamp로 끝을 모아 traction 하면서 상부 식도 bed를 thoracic inlet 까지 박리하여 모두 mobilization 하였다.
Tracheal retractor를 trachea에 걸어 양손으로 traction 하면서 aortic arch의 상방에서 위쪽으로 주행하고 있는 Lt recurrent laryngeal nerve 를 확인하고 LN group을 채취하였다. Dissection bed는 surgicel을 부착하여 bleeding control을 하였다. Tracheal retractor를 내려놓고 lung retractor를 right main bronchus에 걸어 lung 과 같이 anterior 쪽으로 traction 하여 subcarinal region을 노출시켜 LN7 group을 박리하였다. Upper thoracic esophagus의 anastomosis 할 부위에 prolene 2-0를 이용해 purse-string suture 한 뒤 rubber tipped mosquito clamp로 이 실을 잡아두었다. Purse string 1cm 하방에 bovie electrocautery로 esophagus에 vertical incision을 넣었다. Mucosa layer를 포함하여 esophagus의 whole layer를 잡아 양쪽으로 벌리고 L-tube 를 마취과에 지시해 20cm까지 withdrawal 하였다. Black-silk 2-0로 purse string suture 아래의 vertical incision 끝에 tagging suture를 하였다. Betadine ball 2로 lumen 안을 닦아낸 다음 EEA 28mm Anvil을 삽입한 후 purse-string 직하방에서 curved Metzenbaum scissor를 이용하여 esophagus를 절단하였다. 이때 tagging suture도 같이 제거했다.
Thoracic esophagus의 transection margin을 gauze로 감싼 다음 azygos arch 아래로 통과시켜 밖으로 깨낸 다음 1st assistant가 mucosa와 submucosa를 포함하여 양 끝으로 잡고 그 끝을 잘라 proximal resection margin으로 frozen biopsy를 보냈다. 남은 식도는 절단면을 surgeon이 betadine ball로 소독한 후 gauze로 감싸 Kelly clamp를 물어두었다. 식도를 조심스럽게 끌어 올려 위를 흉강 내로 위치시켰다. 식도 끝을 다시 깨끗한 gauze로 감싼 다음 azygos arch 아래로 통과시키고 cardia와 식도 경계에 tagging suture를 하였다. Tagging suture 상방으로 Bovie electrocautery 를 이용하여 gastric tube 의 cardia를 절개하여 내부를 povidone ball로 닦은 다음 tagging suture를 끌어올리면서 EEA 본체를 안으로 밀어넣었다. 본체의 knob을 반시계방향으로 돌려 본체에서 Trocar를 돌출되게 한 다음 gastric tube 내강에서 밖으로 trocar를 관통시켰다. 이 때 Anvil과 결합 시키고 보넻의 knob을 다시 녹색 indicator가 나타날 때까지 시계 방향으로 돌린 후 fire 하여 esophagogastrostomy를 완성하였다. 다시 knob을 반시계 방향으로 돌려 Anvil을 풀어 gastric tube 절개창을 통해 빼냈다. Anvil 내의 proximal resection margin (true resection margin) 을 blade로 purse string 실 부위를 눌러서 제거한 후 mucosa 를 도려내어 resection margin (#2)로 다시 frozen biopsy 검체로 보냈다. Gastric conduit 절개창을 통해 anastomosis site를 확인하고 L-tube를 50cm 까지 밀어 넣고 고정하였다. Gastric tube 절개창 부위를 TA 90로 stapling 하고 tagging suture와 함께 stump 바깥쪽을 절제하였다. Esophagogastrostomy site는 vicryl 3-0로 interrupted lambert suture를 하여 보강하였다. Azygos arch 위쪽에서 세군데를 vicryl 3-0 suture를 이용하여 mediastinal pleura 양쪽과 gastric tube의 seromuscular layer를 관통시켜 고정하였다. Azygos arch 아래쪽에서도 같은 방법으로 고정하였고 Azygos vein 근처에서 mediastinal pleura와 staple margin을 같이 suture 하여 고정하였다. Azygos arch를 ligation 하여 묶어두었던 실 각각을 모아 tie하였다. Warm normal saline을 흉강 내에 채우고 irrigation 하고 parenchymal airleak이 발견되는 부위를 확인하였다. 28fr straight chest tube를 8th ICS PAL을 통해 삽입한 후 layer by layer로 wound closure 하였다. Extubation 한 이 후 vital sign을 monitoring 하면서 환자를 TS ICU로 이송하였다.